
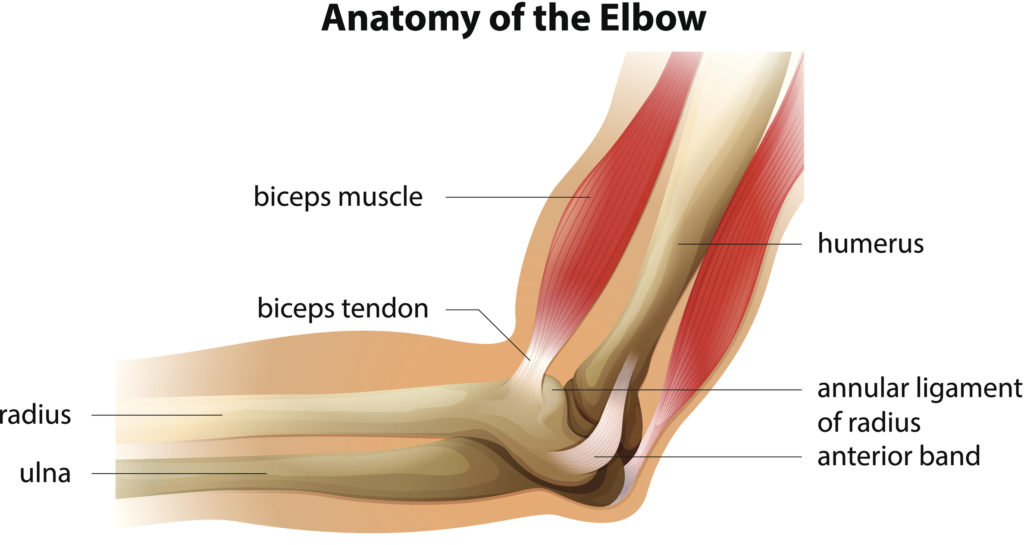
Illustration showing the anatomy of the elbow
The biceps muscle of your arm has two tendons that come off the top end of the muscle and attach to different parts of the scapula and then then one tendon at the bottom end that attaches down near the elbow onto the radius bone in the forearm. The biceps acts to supinate your forearm (turns your palm up) and also to flex (bend) the elbow.
If inflamed or torn, the biceps can cause pain in the front of one’s shoulder. Some patients I see in the office also complain of snapping or catching in the front of the shoulder. On physical exam, the patient often has very well localized pain over the biceps tendon in the groove that it normally sits in along the front and top of the humerus. Treatment initially consists of physical therapy, activity modification, ice, and sometimes a steroid injection around the inflamed tendon. If these measures fail to provide long term relief, then an MRI of the shoulder is indicated to rule out a tear or subluxation of the biceps tendon out of the groove where it normally sits.
If an MRI reveals that the biceps tendon is torn or subluxated, then patients often come to surgery as the tendon will not heal and a torn or subluxated tendon can cause further damage, namely tearing of the adjacent rotator cuff tendon, the subscapularis. In lower demand, older patients, consideration can be given to simply surgically releasing the tendon from its attachment in the shoulder joint and letting the tendon fall down the arm slightly to then scar in. This procedure is called a biceps tenotomy. Studies show that the majority of older patients do fine with no long term pain and good function after biceps tenotomy.
Some patients actually present to me with a ruptured biceps tendon. Depending on the patients age and activity, this can often be treated without any surgery as long as there is not an associated rotator cuff tendon tear. A certain famous Broncos quarterback actually ruptured his biceps tendon while playing for the Broncos some years ago, and he did well with no further treatment for it. In the office, I would recommend that an older patient who ruptures their tendon just let it heal.
However, if a patient is in surgery for their shoulder, I recommend not just releasing the biceps tendon but anchoring it to the bone (called a biceps tenodesis), especially if the patient is young and active. The advantages of fixing or anchoring the tendon to the bone are that in patients who have had their biceps simply released, there is a cosmetic deformity (the so-called Popeye deformity with the muscle being bunched up farther down the arm), there is a slight loss of strength, and there is a higher instance of crampy pain and fatigue in the biceps when lifting or using the arm. Finally, when the biceps is torn or subluxated, there is often a tear of the adjacent subscapularis rotator cuff tendon which needs to be repaired as well.
In throwing athletes and in people who do a lot of overhead work or overhead sports, SLAP tears can occur. A SLAP tear is a tear of the labrum from the top of the shoulder socket (I liken the labrum to a rubber gasket that surrounds the socket of the shoulder joint). The biceps tendon attaches into the top of the labrum and is the biceps is frequently torn along with the labrum. SLAP tears do not heal on their own but they may become less painful by modifying activities. I prescribe physical therapy and many patients will not need surgery for a SLAP tear. However, if pain persists, these are fixed arthroscopically often by doing a biceps tenodesis (removing the biceps from the torn and unstable labrum and then anchoring the biceps to the bone further downstream) and shaving and smoothing the labral tear depending on the patient age and activity level.